Cranioplasty refers to the operation of filling and repairing the skull defect with various repair materials. It is one of the most routine operations in neurosurgery at present and can be carried out in many primary hospitals. Studies have proved that skull repair can not only restore the shape of the cranial cavity, but also play an important role in restoring the neurological function of patients.
Cranioplasty is a time-honored medical technique that has been practiced by our ancestors for thousands of years. The Museum of Osteology in Oklahoma, USA, has the skull of a warrior in Peru who was wounded in battle 2,000 years ago. A metal plate was inserted into the skull to repair the fracture. With the rapid development of industrial level, scientific technology and diagnostic means, cranioplasty has become a common and routine operation in neurosurgery. In this process, the skull repair material also goes through the following stages:
Xenogeneic bone material: In 1668, doctor vanMeekeren used dog bone tissue to repair a human skull defect, the first documented xenogeneic bone graft in the world. Subsequently, bone tissue transplantation from apes, rabbits and cows was introduced into humans. In addition to the common complications such as infection and bone absorption after transplantation, xenograft often causes secondary injuries to patients due to the great immune rejection of xenograft materials by the human body. Therefore, xenograft materials are no longer used in clinical skull repair .

Autogenous bone transplantation: In 1821, doctor Vonwalther performed the world’s first autogenous bone transplantation to repair skull defects, and doctor Lollier proposed the important role of periosteal membrane in bone regeneration in 1867. Subsequently, a large number of literatures have been reported on the repair of skull defects by autologous cranial flap, external mandibular plate, rib, iliac crest and fibula flap. Autologous rib made into strips or powder is suitable for repairing small skull defect. At present, autologous bone repair is still the gold standard for skull reconstruction. Autologous bone tissue has good bone conductivity and histocompatibility, no rejection reaction, and low rate of bone exposure after surgery. However, there are some problems such as limited donor area, difficulty in shaping, increased secondary trauma, and high bone absorption rate of bone graft, so the clinical application is limited.
Allogeneic bone: The large number of World War I and World War II soldiers with skull defects due to gunfire and explosions led to significant advances in the repair of skull defects. In the early 20th century, there were reports of skull defects repaired by human cadaver skull transplantation. Allograft materials are usually derived from other people’s bone flap, which can solve the problem of insufficient autogenous bone in patients with large skull defect area to a certain extent, and meet the clinical needs. In order to reduce rejection, radiation and autoclave sterilization are commonly used to treat allograft bone. Because the acquisition of allogeneic materials will cause great trauma to the donor and involve many ethical issues, they are rarely used at present.
Polymer materials: bone cement, hydroxyapatite, silicone rubber.
Bone cement: Polymethyl methacrylate (PMMA) is a material that is strong, stable, heat-resistant, and X-penetrable. It is also called bone cement because it is similar in strength to human bone. However, it is brittle and easy to crack when external force hits, so it is rarely used alone in skull repair. Compared with autogenous bone, poly (methyl methacrylate) lacks pores and cannot be infiltrated and wrapped by new tissue after implantation into the intracranial, which is prone to infection after surgery. So, it has been rarely used at present. In addition, it is not used as a repair material for skull defects in children because it is not compatible with surrounding tissue and does not grow with the skull.

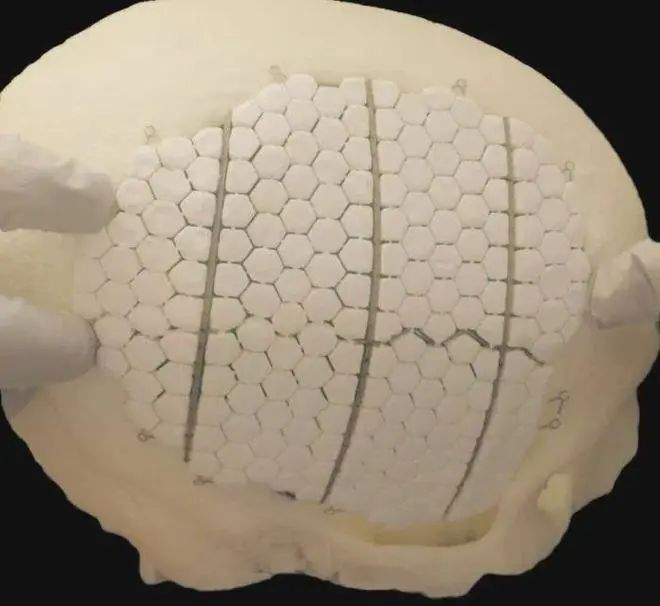
Hydroxyapatite: Its molecular structure and calcium phosphorus ratio are very similar to the inorganic components of normal bone, belonging to calcium phosphorus ceramics. Hydroxyapatite has good biocompatibility, bone conductivity and bone induction. After implantation in the body, calcium and phosphorus will dissociate from the surface of the material and be absorbed by body tissues, and induce the growth of new bone tissues. Through CAD/CAM technology, hydroxyapatite can be prefabricated into personalized implant body according to the size and shape of the defect before surgery, but the main problem is that intraoperative screw fixation and postoperative external force are easy to make the fracture, and the postoperative infection rate is high. Moreover, hydroxyapatite degrades too quickly in vivo, so it is usually used to repair small bone defects left by skull drilling, and large skull defects need to be fixed with titanium mesh.
Silicone rubber: is a kind of non-metallic material widely used in skull repair at the end of last century, it has the advantages of easy cutting and fixing, good tissue compatibility, low price and so on. But its disadvantage is that the material is thick, soft texture, poor strength and the edge is not easy to stick and easy to warping, material instability is easy to cause subcutaneous hydrops or infection, shift up warping and exposed. It is difficult to use silicone to repair even if the stability of any long-term support effect, so silicone rubber is gradually phased out.
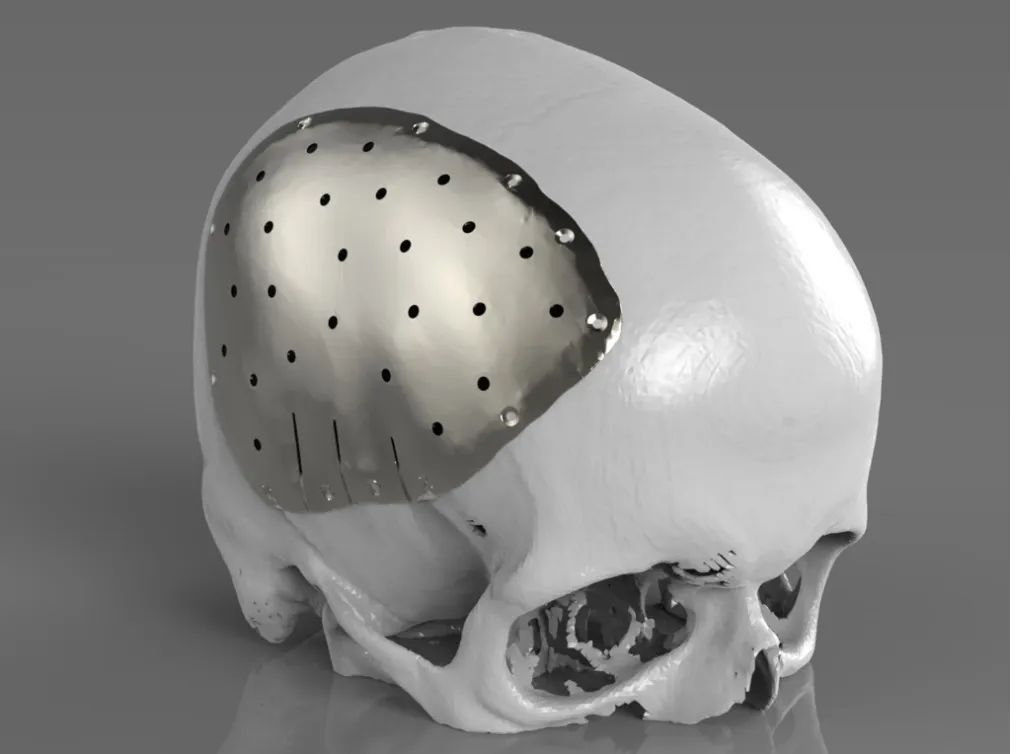
Metal transplantation materials: The metals used for skull repair mainly include gold, silver, aluminum, titanium, etc. Aluminum is no longer used as a metal in bone grafts, which dissolves over time and can irritate nerve tissue in the brain, causing seizures. Although gold is effective as a repair material, it is soft and not cost-effective, so it has not been widely used. The skull repaired with silver plate is prone to oxidation reaction with tissues around the skin, resulting in discolor of the skin flap. Moreover, sterling silver is soft and has poor resistance to external forces, resulting in deformation after stress, thus damaging intracranial tissues and nerves. Titanium began to be used in cranioplasty in the 1950s. The material made of titanium is safe, strong, acid and alkaline, and rarely produces rejection reaction in the human body, so it is widely used in clinic. However, titanium has high brightness in postoperative CT or MRI imaging, and it is difficult to determine if hematoma or tumor occurs near postoperative intracranial implants. In addition, titanium is a metal material with good heat transfer, which may cause damage to intracranial brain tissues and nerves in the outdoor high temperature environment. Therefore, titanium is still not the most ideal material choice for cranioplasty.
Polyether–ether–ketone material: Polyether-ether-ketone(PEEK), as a semi-crystalline linear polycyclic aromatic linear polymer, was first used in clinical implants in 1998, mainly focused on spinal and hip replacement in the early stage. Due to its excellent properties in the combination of strength, durability, stiffness and resistance, its use in clinical medicine has been expanding. In 2007, PEEK material was first reported in the reconstruction of fronto-orbital defect in maxillofacial surgery, which made it gradually known to neurosurgeons. The advantages of PEEK materials are mainly that the elastic and strength thresholds are very close to cortical bone, making it a valuable choice for reconstruction of skull defects. PEEK has the strength and hardness similar to cortical bone. It is inert and basically excludes the release of cytotoxic substances caused by mechanical or chemical decomposition factors. In addition, due to the structural stability of the polyether ether ketone material at high temperatures, it can be sterilized under wet or dry heat without deformation. Its extremely low thermal conductivity reduces the possibility of external temperature changes causing damage to intracranial brain tissue and nerve tissue, and does not affect the imaging results of patients. In addition, the polyether ether ketone material can also be combined with CT thin layer scanning and computer 3D printing technology to make the forming material with the biological curvature of the patient’s skull defect almost exactly the same, making the skull more beautiful after repair. However, the price of polyether ether ketone material is high, which is difficult for some patients to accept. Therefore, regardless of the price factor, polyether ether ketone material is considered to be the most ideal material for cranioplasty.
Medical implanting grade polyether ether ketone (PEEK) material independently developed and produced by Guangzhou Junsun Medical Technology Co., LTD has excellent performance and low price, which is suitable for the repair and implantation of skull defects.